Mental Health Services Act MHSA Full Text
|
Special Note: CALBHB/C is advocating for a standard set of MHSA Performance Outcome Data. CALBHB/C Issue Brief; Letters To: MHSOAC and DHCS & Senate Subcommittee. Also see NAMI CA MHSA Position Paper, CSAC Recommendations
Mental Health Services Act Training Modules:
The Mental Health Services Act (MHSA) of 2004 passed by the voters as “Proposition 63,” increased overall State funding for the community mental health system by imposing a 1% income tax on California residents with more than $1 million per year in income. The stated intention of the proposition was to “transform” local mental health service delivery systems from a “fail first” model to one promoting intervention, treatment and recovery from mental illness. A key strategy in the act is the prioritization of prevention and early intervention services to reduce the long-term adverse impacts of untreated, serious mental illness on individuals, families and state and local budgets. All MHSA projects and programs shall be planned, developed, approved, implemented, monitored and updated through a community stakeholder process.
According to WIC 5813.5, MHSA Planning for services shall be consistent with the philosophy, principles, and practices of the Recovery Vision for mental health consumers:
According to WIC 5813.5, MHSA Planning for services shall be consistent with the philosophy, principles, and practices of the Recovery Vision for mental health consumers:
- To promote concepts key to the recovery for individuals who have mental illness: hope, personal empowerment, respect, social connections, self-responsibility, and self-determination.
- To promote consumer-operated services as a way to support recovery.
- To reflect the cultural, ethnic, and racial diversity of mental health consumers.
- To plan for each consumer's individual needs.
Role of Mental Health Board"County mental health programs shall prepare and submit a Three-Year Program and Expenditure Plan (Plan) and Annual Updates for Mental Health Service Act (MHSA) programs and expenditures" (Welfare and Institutions Code Section (WIC) § 5847)
It is important to understand the roles of the MHB, the Mental/Behavioral Health Director and the Board of Supervisors (or Governing Body).
...(b) ... (a). Each adopted three-year program and expenditure plan and update shall include any substantive written recommendations for revisions. The adopted three-year program and expenditure plan or update shall summarize and analyze the recommended revisions. The mental health board shall review the adopted plan or update and make recommendations to the local mental health agency or local behavioral health agency, as applicable, for revisions. The local mental health agency or local behavioral health agency, as applicable, shall provide an annual report of written explanations to the local governing body and the State Department of Health Care Services for any substantive [see (f) below] recommendations made by the local mental health board that are not included in the final plan or update. (f) For purposes of this section “Substantive recommendations made by the local mental health board” means any recommendation that is brought before the board and approved by a majority vote of the membership present at a public hearing of the local mental health board that has established its quorum. (WIC 5848 updated 10/19) See "Best Practices" Manual for more info. |
Six ComponentsMHSA funds are divided into six components. County mental health agencies are required to develop detailed plans for the use of MHSA funds in each of these components, then submit those plans to the CA Department of Health Care Services or Mental Health Services Oversight and Accountability Commission (MHSOAC) or State for approval. The following are the components.
1) Community Program Planning: One-Pager: (CPP: Definition, Participants & Process) Community Community Program Planning (CPP) is the state-mandated, community collaboration process that is used to: assess the current capacity, define the populations to be served and determine strategies to provide effective MHSA-funded programs that are:
CCR, 9 CA ADC § 3200, 3200.060, 3200.270, 3200.90, 3300, 3315, 3320) and WIC 5848(a) . 2) Community Services and Supports (CSS) CSS is the largest funding component of MHSA and is intended to expand and transform services for children, youth, adults and older adults living with serious mental illness, with an emphasis on culturally competent and recovery-oriented services. Additionally, CSS funding focuses on consumer and family driven services, community collaboration and integration of services. CSS services include Full Service Partnership (FSP) programs of which 51% of the CSS funding is mandated. In addition to FSP programming, the CSS component includes General Systems Development which is used to enhance the system of care and Outreach and Engagement to increase access to unserved/underserved communities as determined by the County penetration rates. CSS funds may also be used to provide housing support for mental health consumers with serious mental health conditions. County MHPs have three years to spend CSS funds. 3) Prevention and Early Intervention (PEI): The goal of PEI is to help counties implement services that promote wellness, foster health, and prevent the suffering that can result from untreated mental illness to include: (1) Outreach to families, employers, primary care health care providers, and others to recognize the early signs of potentially severe and disabling mental illnesses. (2) Access and linkage to medically necessary care provided by county mental health programs for children with severe mental illness, as defined in Section 5600.3, and for adults and seniors with severe mental illness, as defined in Section 5600.3, as early in the onset of these conditions as practicable. (3) Reduction in stigma associated with either being diagnosed with a mental illness or seeking mental health services. (4) Reduction in discrimination against people with mental illness. (c) The program shall include mental health services similar to those provided under other programs effective in preventing mental illnesses from becoming severe, and shall also include components similar to programs that have been successful in reducing the duration of untreated severe mental illnesses and assisting people in quickly regaining productive lives. (d) The program shall emphasize strategies to reduce the following negative outcomes that may result from untreated mental illness: (1) Suicide. (2) Incarcerations. (3) School failure or dropout. (4) Unemployment. (5) Prolonged suffering. (6) Homelessness. (7) Removal of children from their homes. At least 51% of the PEI funding must be used for programs and services dedicated to children and youth under the age of twenty-five. Related Legislation 4) Innovation: The goal of Innovation is to increase access to underserved groups, increase the quality of services, promote interagency collaboration and increase access to services. Counties select one or more goals and use those goals as the primary priority or priorities for their proposed Innovation plan. “Innovation projects are novel, creative and/or ingenious practices/approaches that contribute to learning and that are developed within communities through a process that is inclusive and representative, especially of unserved, underserved and inappropriately served individuals” Innovation Projects are required to: A. Introduce a mental health practice or approach that is new to the overall mental health system, including, but not limited to, prevention and early intervention, or B. Make a change to an existing practice in the field of mental health, including but not limited to application to a different population, or C. Apply to the mental health system a promising community-driven practice or approach that has been successful in non-mental health contexts or settings. County MHPs have three years to spend each annual INN allocation (five years for Counties with population 200,000 or less). The MHSOAC controls funding approval for the Innovation (INN) component of the MHSA. 5) Capital Facilities and Technology Needs (CFTN): The CFTN component works towards the creation of a facility that is used for the delivery of MHSA services to mental health clients and their families or for administrative offices. Funds may also be used to support an increase in peer-support and consumer-run facilities, development of community-based settings, and the development of a technological infrastructure for the mental health system to facilitate the highest quality and cost-effective services and supports for clients and their families. 6) Workforce Education and Training: The goal of the Workforce Education & Training (WET) and WET Regional Partnerships component is to develop a diverse workforce, with the following goals:(1) Addressing identified shortages in occupations, skill sets, and individuals with unique cultural and linguistic competence in urban and rural county mental health programs and private organizations providing services in the Public Mental Health System; and (2) Education and training for all individuals who provide or support services in the Public Mental Health System, to include fostering leadership skills. This education and training contributes to developing and maintaining a culturally competent workforce, to include clients and family members who are capable of providing client and family-driven services that promote wellness, recovery and resilience, and lead to measurable, values-driven outcomes. Regional partnerships are an important part of WET because schools and training sources serve individuals across county lines. For example, community colleges, universities, graduate and professional programs serve individuals across various geographic regions of California. |
Fiscal Information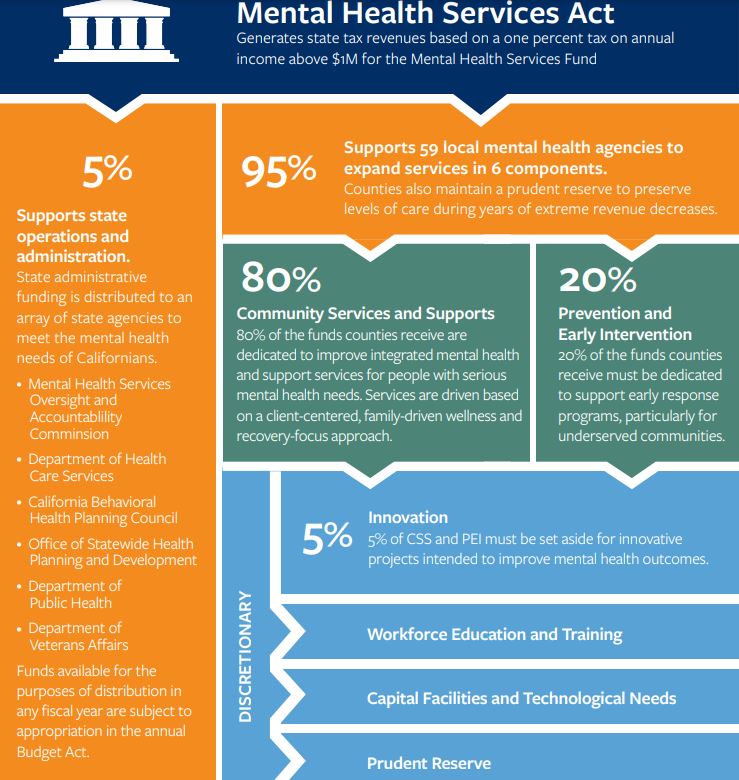
By law, the State allocates MHSA funds from the Mental Health Services Fund (MHSF) to County Mental Health Plans (MHPs)[1] for three components: Innovation (INN), Prevention and Early Intervention (PEI) and Community Services and Supports (CSS).
TIMEFRAMES: 3 Years: CSS, PEI, and INN components must be spent within three years (or within five years for INN for Counties with population 200,000 or less). 10 Years: Capital Facilities and Technological Needs (CFTN), Workforce Education and Training (WET) and WET Regional Partnerships must be spent within ten years of allocation. UNSPENT FUNDS: The law requires any unspent MHSA funds held by County MHPs to be kept in interest-bearing accounts. County MHPs are required to treat any interest earned as additional revenue for the specific component. County MHPs have differed in their use of interest earned. Some have spent it as it is earned while others have allowed interest to accumulate as a cash reserve. Funds not spent within their mandated timeframes are to be returned to the State for re-allocation to County MHPs, a process called "reversion". Prudent Reserve funds are not time limited and are meant to remain permanently with the County MHP until needed. ON-LINE DATA: Annual Revenue and Expenditure Information is available from the CA Department of Health Care Services (DHCS) website: https://www.dhcs.ca.gov/services/MH/Pages/MHSA-Fiscal-Oversight.aspx . [1] In California, Medi-Cal mental health waivers establish MHPs, which have the responsibility to provide psychiatric inpatient hospital services and outpatient specialty mental health services within their region. The 59 County MHPs include 57 county regions (including Sutter and Yuba Counties combined as one region) along with two city regions, including the City of Berkeley and Tri-City (Pomona, Claremont and La Verne within Los Angeles County). [2] Once funds are received, County MHPs are permitted to meet local needs by transferring funds from CSS to three other components: Capital Facilities and Technological Needs (CFTN), Workforce Education and Training (WET) and WET Regional Partnerships. Counties also are permitted to transfer some portion of CSS funds to a Prudent Reserve account, a "rainy-day" fund used to protect levels of service when MHSA funding is not sufficient to support ongoing programming. Counties are permitted to allocate up to 33% of the five-year average of revenue under the Community Services and Supports component to the Prudent Reserve (PR) fund with stakeholder endorsement and provided the current MHSA Three-Year Integrated Program & Expenditure Plan includes the identification of PR funds. The purpose of maintaining PR funds is to safeguard programs and services in the event that there is a budget crisis. * * * * * * * * * * * * * * * More information on how California funds mental health: Mental Health Funding Explained, CA Hospital Assoc. 2016 |
T